

















 38 / 48
38 / 48

80
VOLUME 12 NUMBER 2 • NOVEMBER 2015
RESEARCH ARTICLE
SA JOURNAL OF DIABETES & VASCULAR DISEASE
of Obafemi Awolowo University Teaching Hospitals complex
(OAUTHC), Ile Ife, Nigeria. Ethical clearance for the study was
approved by the Ethics and Research Committee of the Hospital
in conformity with ethical guidelines of the 1975 Declaration of
Helsinki, and all participants gave written consent to participate.
Demographic parameters of the subjects were noted and
recorded. All subjects were clinically examined to evaluate their body
mass index (BMI) and cardiovascular status at rest. Subjects were
considered diabetic if they had fasting plasma glucose (FBG) values
≥ 126 mg/dl (7.0 mmol/l)
8
or if they used hypoglycaemia medication.
Fasting plasma glucose and two-hour post-prandial plasma glucose
(2HPP) values were obtained 24 hours prior to the procedures.
A resting 12-lead ECG was done to exclude patients with
baseline ST-segment abnormalities and bundle branch block. Also
excluded were patients with coexisting hypertension or who were
on antihypertensive(s), those with established chronic renal failure
or serum creatinine levels > 1.5 mg% (132 μmol/l), congestive
heart failure, valvular heart disease and other diseases known to
influence LV function, such as thyroid disease and severe obesity.
All the subjects underwent treadmill-symptom limited maximal
exercise using the Bruce protocol.
9
The protocol continued until
one of several endpoints was reached. These included if the patient
achieved the age-predicted maximum heart rate; requested that the
exercise be terminated; developed severe chest pain, fatigue, leg
discomfort or dyspnea; developed frequent premature ventricular
beats; developed a systolic blood pressure > 250 mmHg or a drop
in the pre-test systolic blood pressure > 10 mmHg; or developed
any other problems necessitating termination of exercise.
The subjects also had transthoracic two-dimensional (2D) and
2D derived M-mode echocardiography performed, according to
standard procedure,
10
with simultaneous electrocardiographic
recordings while in the left lateral decubitus position, using a
standard ultrasound machine (Sonoline G60S Ultrasound Imaging
System) with 4.2-MHz transducer. Left ventricular enddiastolic
measurements were taken during at least three cycles
11
and
included left ventricular internal diameter (LVIDD), posterior wall
thickness (PWT) and interventricular septal thickness (IVST). Left
ventricular mass was estimated from the American Society of
Echocardiography’s formula
11
:
Estimated LV mass index (g/m
2
) = 0.80 [1.04 (LVIDD + PWT +
IVST)3 – (LVIDD)3] + 0.6 g/BSA
Upper normal limits for LV mass index were 134 and 110 g/m
2
in men and women, respectively.
12
Relative wall thickness (2 ×
posterior wall thickness/LV diastolic diameter) was calculated.
13
A partition value of 0.45 for relative wall thickness was used for
both men and women.
14
Patients with increased LV mass index
and increased relative wall thickness were considered to have
concentric hypertrophy, and those with increased LV mass index and
normal relative wall thickness were considered to have eccentric
hypertrophy. Those with normal LV mass index and increased or
normal relative wall thickness were considered to have concentric
remodelling or normal geometry, respectively.
Results
The diabetic subjects and controls had comparable ages and BMIs
(48.37 ± 6.96 vs 48.35 ± 6.13 years;
p
= 0.197 and 24.82 ± 3.66
vs 24.38 ± 1.94 kg/m
2
;
p
= 0.861, respectively). Diabetic subjects
had significantly higher FBG values than the controls (8.94 ± 2.13
vs 4.75 ± 0.37 mmol/l;
p
≤ 0.001).
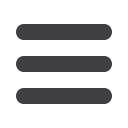
As shown in Table 1, normotensive diabetic subjects had higher
exercise-induced haemodynamic parameters of peak systolic (pSBP)
and peak diastolic blood pressure (pDBP) but lower peak heart
rates (pHR). There was no statistically significant difference in left
ventricular mass index (LVMI). Nineteen (29.7%) and 11 (17.2%)
normotensive diabetic subjects had normal left ventricular geometry
and concentric left ventricular remodelling, respectively. None of
the normotensive diabetic subjects had concentric or eccentric left
ventricular hypertrophy. Thirty (46.8%) and four (6.3%) controls
had normal left ventricular geometry and concentric left ventricular
remodelling, respectively. None of the subjects had concentric or
eccentric left ventricular hypertrophy.
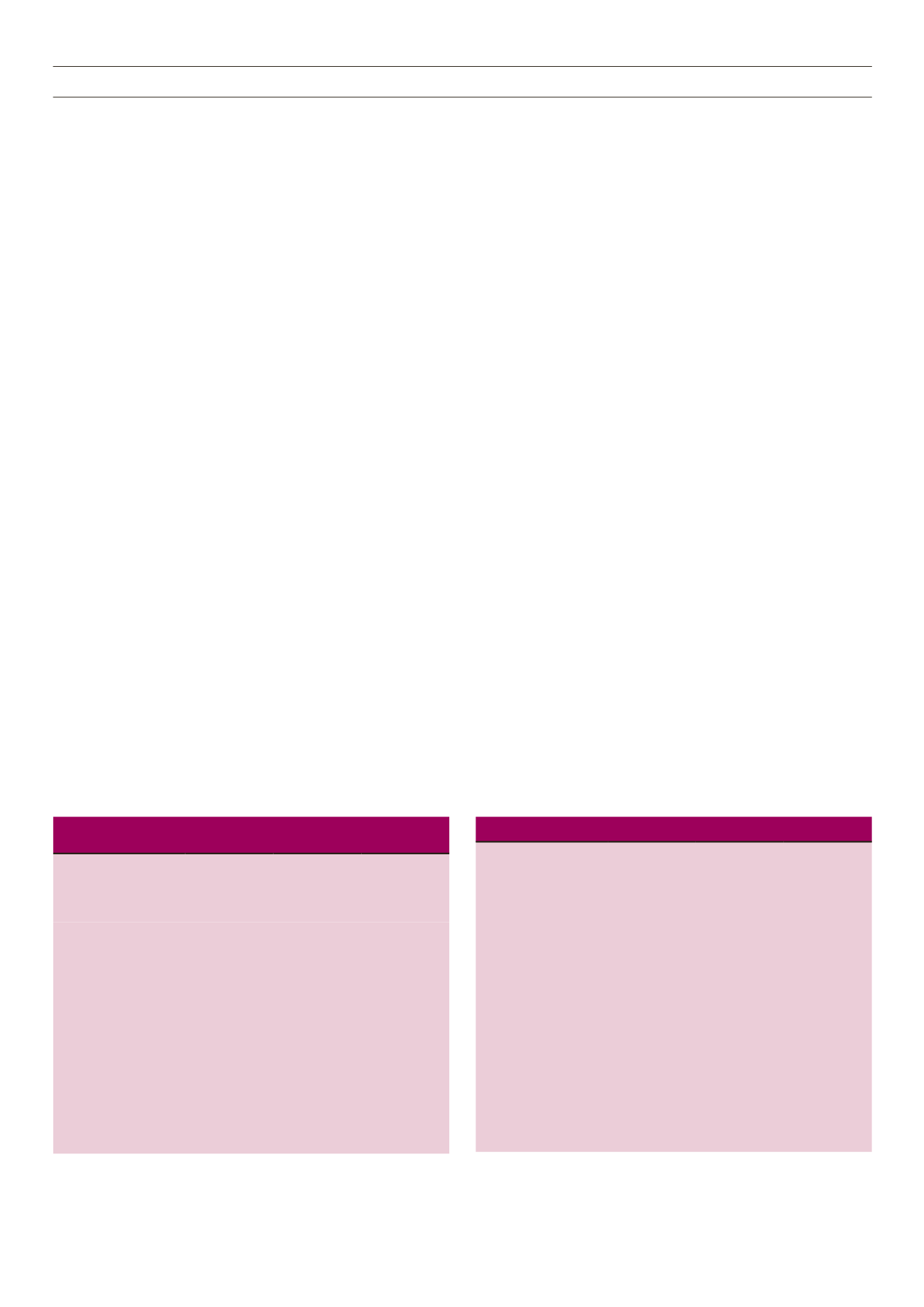
The normotensive diabetic subjects were then divided into two
groups: G1 (normal) and G2 (concentric left ventricular remodelling)
on this basis. The groups had comparable mean ages, BMIs, FBG
and two-hour post-prandial blood glucose values, heart rates,
and SBP and DBP at rest (Table 2). G2 patients had a higher mean
duration of diabetes than G1 (69.0 ± 9.48 vs 18.7 ± 8.7 months;
p
Table 1.
Haemodynamic response and echocardiographic pattern of
the study population
Parameters
Normotensive
diabetics
(
n
= 30))
Controls
(
n
= 34)
p
-value
(Student’s
t
-test)
rHR (per min)
91.37 ± 16.10 83.29 ± 5.36
0.038
rDBP (mmHg)
73.03 ± 5.46 71.94 ± 3.13
0.713
rSBP (mmHg)
117.13 ± 6.36 113.62 ± 4.51
0.044
pHR (per min)
166.00 ± 15.61 179.03 ± 9.10 < 0.001
pDBP (mmHg)
95.67 ± 9.35 89.12 ± 7.12
< 0.001
pSBP (mmHg)
205.00 ± 18.15 185.41 ± 10.81 < 0.001
Exercise capacity (METs)
8.07 ± 1.47 8.11 ± 0.88
0.992
LVMI (g/m
2
)
93.97 ± 17.04 90.55 ± 17.09
0.512
IVST (mm)
10.24 ± 1.36 9.45 ± 1.44
0.084
PWT (mm)
9.70 ± 1.51 9.43 ± 1.50
0.771
RWT
0.45 ± 0.68 0.41 ± 0.07
0.038
Statistical significance at
p
< 0.05;
Values are expressed as mean ± SD;
rHR = resting heart rate, pHR = peak heart rate.
Table 2.
Clinical and demographic pattern of G1 and G2 subjects
Parameters
Normal LV
geometry
(
n
= 19)
Concentric
LV remodelling
(
n
= 11)
p
-value
(Student’s
t
-test)
Age
48.68 ± 7.7 47.82 ± 5.7
0.749
Gender
M: n (%))
7 (36.8%)
8 (72.7%)
0.058*
F: n (%)
12 (63.2%)
3 (27.3%)
BMI (kg/m
2
)
24.8 ± 4.1
24.8 ± 2.9
0.992
Duration of diabetes
(months)
18.7 ± 8.7
69.0 ± 9.48
0.007
FBG (mmol/l)
9.8 ± 2.03
8.1 ± 1.9
0.082
2HPP (mmol/l)
12.2 ± 1.9
13.8 ± 3.5
0.236
rHR (bpm)
92.1 ± 18.2 90.1 ± 12.4
0.748
rDBP (mmHg)
72.4 ± 5.8
74.2 ± 4.9
0.390
rSBP (mmHg)
118.5 ± 6.5 114.7 ± 5.6
0.116
rPP (mmHg)
46.2 ± 8.7
40.6 ± 3.9
0.052
Statistical significance at p < 0.05;
*Chi-square. Values are expressed as mean ± SD