


















 21 / 44
21 / 44

VOLUME 14 NUMBER 1 • JULY 2017
19
SA JOURNAL OF DIABETES & VASCULAR DISEASE
DIABETES CARE MODEL
the clinic is the introduction of electronic medical records (EMR).
EMR serve important roles in ensuring more complete and accurate
documentation by the clinicians working at the clinic, and secondarily
help as a data-collection tool for research and auditing purposes.
21
In this study we propose a model for a diabetes clinic, which
addresses all of the above facets of DM patient care. This model
can be applied to other resource-limited clinics in other developing
world settings. We begin by describing the clinic at Edendale as it
was (it is likely to be similar to many other diabetes clinics across
the developing world), and then describe implementation of the
multifaceted and holistic approach to patient care.
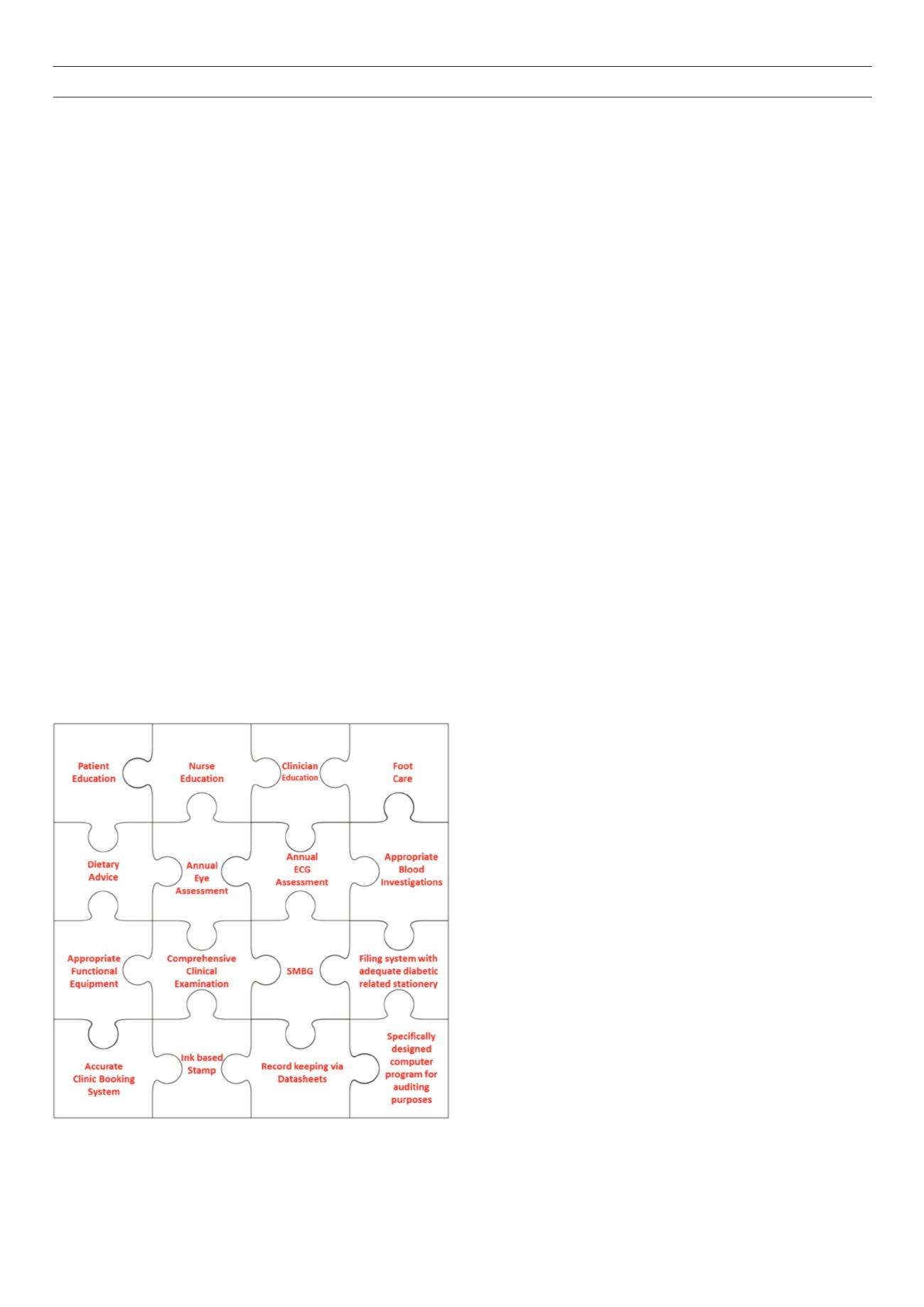
Optimal care of the diabetic patient, whether in resource-
poor or well-resourced facilities, requires an integrated package
of services geared towards holistic care of the patient. Fig. 1 is a
diagrammatical representation of the steps implemented in the
diabetes clinic, where each step of this process or ‘piece of the
puzzle’ is interdependent on the other to ensure maximal effect on
the outcomes of DM and its complications.
The clinic as it was
Before the implementation of the holistic integrated approach to
diabetes care, the situation at Edendale diabetes clinic mirrored
many in resource-poor areas. Edendale Hospital is a busy regional
hospital situated in Pietermaritzburg, KwaZulu-Natal. Historically
this resource-limited diabetes clinic had a poor booking system,
which resulted in about 60 to 70 patients being consulted on one
day per week.
Patients who were consulted had only their blood pressures (BP)
taken and random blood glucose levels (RBG) determined prior to
consulting one of the two doctors stationed at the diabetes clinic
for the month. With such great numbers of patients and only
two doctors in the clinic, most management decisions were made
based on only the BP and RBG readings, with very little or no time
spent on patient education or patient examination. Management
decisions were made by the individual doctor at most times without
any reference to local standardised diabetes guidelines. There was
a lack of continuity of clinical care as these doctors were rotated
on a monthly basis.
The clinic facility, being in a resource-limited environment, lacked
adequate equipment for height, weight and waist measurements,
and urine dipsticks were only performed if patients presented to
the clinic with an RBG > 20 mmol/l, and then looking for ketonuria
only. The two rooms used for this busy clinic run on Wednesdays
were used for other clinics for the rest of the week. The correct
stationery/forms specific to diabetes care were therefore always in
short supply and, if present, difficult to locate. No tuning forks,
patellar hammers or monofilament testing equipment were
available at the clinic. The wall-mounted ophthalmoscopes in both
rooms were non-functional.
This description of the clinic probably reflects a typical diabetes
clinic service run in most similar hospitals in the country.
Changes implemented
Having assessed the diabetes clinic in this resource-limited hospital,
the following changes were introduced in an integrated manner to
improve overall diabetes care.
Physical facilities
Three rooms for the running of the diabetes clinic were allocated and
clearly labelled for dedicated use. Being permanently allocated for
this purpose, they could be equipped and locked when not in use.
Equipment
Equipment such as tuning forks, patellar hammers, monofilaments
and a body mass index (BMI) scale was donated for use in the clinic.
New ophthalmoscopes were provided.
Patient education
Patient education material in the form of posters was acquired and
displayed for easy patient reading while waiting. A diabetes nurse-
educator was employed and stationed at the clinic. In conjunction
with the sessional family physician, patient education sessions are
conducted while patients wait for their vital signs to be recorded.
Staffing
A multidisciplinary clinical team was set up to address all aspects
of diabetes care and includes the following members: specialist
physician, family physician, medical officers, interns, nursing staff,
diabetes nurse-educator, dieticians, podiatrist, and ophthalmologist
for annual review. All members of this team other than the
ophthalmologist are present at the weekly clinics to deliver their
specialised care.
Patients waiting for consultation are allocated to the next
clinician available –the intern, medical officer, family or specialist
physician. Junior clinicians have immediate access to senior doctors
working in the clinic to discuss their patients and issues relating to
their management. Patients who need to consult podiatrists are
identified by the clinicians and then referred accordingly.
A podiatrist plays an integral part in the prevention and
management of diabetic foot complications.
22
After consultation
with the podiatrist, employed by the local tertiary hospital, it was
agreed that she would consult diabetic patients and also provide
weekly group diabetic foot-care education at the clinic.
Fig. 1.
Schematic representation of integrated elements of a comprehensive
and holistic treatment approach to diabetic patients.